South Australian Medical Heritage Society Inc
Website for the Virtual Museum
Home
Coming meetings
Past meetings
About the Society
Main Galleries
Medicine
Surgery
Anaesthesia
X-rays
Hospitals,other organisations
Individuals of note
Small Galleries
Ethnic medicine
- Aboriginal
- Chinese
- Mediterran
Acknowledgments This commentary and the prostheses for photography were kindly provided by Mr. T. Stevenson, Senior Surgeon at the Queen Elizabeth Hospital Department of Orthopaedic Surgery. [This revision 080820]
Hip joint replacement was first used about the end of World War One when attempts were made to replace hips that had been severely damaged by injury or disease with cadaveric or animal bones, but this was before the bodies' immune response to foreign material was understood and these all failed.So, in the 1920s and early 1930s the only surgical option for a severely destroyed hip was arthrodesis (fusion) which gave a painless and strong hip but obviously at the expense of loss of movement.
In the late 1930's following the advance of metallurgy so that relatively inert metal nails, screws and plates could be used for a fixation of fractures, attempts were made to alleviate stiff, painful arthritic hips by inserting metal inter-position discs between the ball and the socket. These were reasonably successful.
In 1947, Austin Moore, an American orthopaedic surgeon in North Carolina , had a patient with a benign tumour in the head of femur (ball in the socket of the hip) and he designed a metal ball with a stem which replaced the diseased bone. [details below]
This worked surprisingly well and over the next few years these hemi-arthroplasties, i.e., replacement of the ball but not the socket in the hip joint were used for patients who had sustained a fracture of neck of femur, a very common injury in an older patient where sometimes the blood supply to the hip is cut off and the bone dies.
In these relatively low demand patients the Austin Moore hemi-arthroplasty got them back on their feet and at least independently mobile. They are in fact still in use today over 60 years later. When used for arthritic hips the result was again only reasonable as of course only the ball had been replaced and there was still the diseased socket.
In the early 1960's Professor Sir John Charnley from Manchester , England who was qualified in Medicine and Engineering designed the first total hip replacement, i.e. replacement of the ball and the socket of the arthritic hip (view here).
His initial materials were a metal ball in a Teflon socket. Teflon had already been used in medicine for hernia repairs and aortic grafts etc, and had been proved to be quite inert and not liable to set off a tissue rejection. However, Teflon moving slowly under weight bearing conditions tended to delaminate and within a few years he changed to the use of high density poly-ethylene as the bearing surface.
This is the material used in roller bearings, conveyor belts, curtain runners etc and has proved a very good bearing surface with a low coefficient of friction and not too much wear.
Fixation of the prosthesis to the bone proved a problem in that many of the early press fit or screw in components ultimately loosened. However, Charnley got around this by the introduction of methyl methacrylate (bone 'cement') which is a material that had been used in dentistry for over twenty years to fix in crowned teeth when the root was intact but the tooth had been broken off. It proved biologically inert.
It is very similar to polyfilla, being a powder and a metal which when mixed together gives off an exothermic reaction and then sets within about 10 or 12 minutes. These cemented hip replacements were first used in the UK in the early 1960's and spread quickly throughout the world.
The first low friction cemented total hip replacements were performed in South Australia in 1968. Good results were obtained almost immediately and there are occasional patients who had hip replacements performed in either the very late 1960's or early 1970's who are still able to walk about on these.
However, they obviously did not and will not last forever and over the years, either wear of the polyethylene or loosening of the bone cement bond led to failure. In the 1980's and 1990's improvements occurred, firstly in the bearing surface where ceramic was used, being a substance which has a good coefficient friction and a very low wear rate.
Also metal on metal, which in the early cases had failed because of the poor metallurgy and tendency to seize when moving slowly under weight bearing conditions, came back into use with better metallurgy and design to allow more lubrication of the surfaces by the tissue fluid.
The fixation to bone also has improved with cement being replaced with very carefully matched porous surfaces which press- fits into the bone without the need of cement and also is now in many cases coated with hydroxylapitite. This is a substance originally obtained from coral which has a very similar structure to bone into which the living bone cells actually grow thinking it is a bit of dead bone and actually osteo-integrate the component to the patient's own bone.
Another more recent advance has been surface replacement where instead of removing the whole head of femur and replacement with a ball and stem, a metal surface is placed over the existing head of femur. This concept came in about 20 years ago, but the initial models failed because of loss of the blood supply to the underlying head of the femur. Newer models seem to have got around this problem.
The current concepts are the use of either surface replacement or hydroxylapitite metal on metal total joint in the young high demand patient, but in the older patient with fewer demands, the somewhat technically easier and substantially cheaper cemented metal and polyethylene replacement is still the treatment of choice.
There are now approximately 20,000 hip replacements performed in Australia each year and the Australian Joint Replacement Registry has records of over 500,000 joint replacements, which are kept and updated so that a very valuable database of joint replacements is available for research and prognostication.
Hip replacement is the most successful type of joint replacement, but the technology has spread to other joints, particularly the knee where replacements are nearly as good as the hips.
The original knee replacements had the same teething problems as hip replacements. Initially the knee was thought to be just a hinge. Early knee replacements were basically just hinges, but the knee in fact is not just a hinge. There is quite a lot of rotation occurring at each step and the early hinges loosened.
These have now been replaced by more anatomical surface replacements usually three or sometimes four components, i.e. a metal component on the end of the femur (thigh bone) a metal component on the top of the tibia (shin bone) with a polyethylene component between these two and sometimes also a polyethylene component on the back of the patella (knee cap).
Joint replacement is also being used in shoulders, elbows, ankles, great toes and knuckles with varying degrees of success.
Nowadays about 95% of patients with joint replacements are pleased with the result. Some of the dissatisfied patients have had obvious problems such as infection, dislocation, thrombosis, etc, but the majority who are unhappy are due to unrealistic expectations — the artificial hip is good but not as good as a normal hip. All possible steps are taken to cut down the risk of infection by ultra-sterile operating conditions, antibiotics, etc and of thrombosis by early mobilisation, anticoagulants, etc.
Even today these large orthopaedic operations do have a small mortality (about 0.3%) mainly as a result of thrombo-embolism (blood clots spreading to the lungs).
Austin Moore Hip Replacement
In 1942 Dr. Moore performed and reported the first metallic hip replacement surgery. The original prosthesis he designed was made of the metal Vitallium. It was about a foot in length. and bolted to the cut end of the femoral shaft. This differs from later (and current) hip replacement prostheses which are inserted within the medullary shaft of the femur. A later version of Dr. Moore's prosthesis, the so-called 'Austin-Moore', is still used today.
Dates Lived: 1899 -1963
Nationality: American
Subspecialty: Joint Replacement Surgery
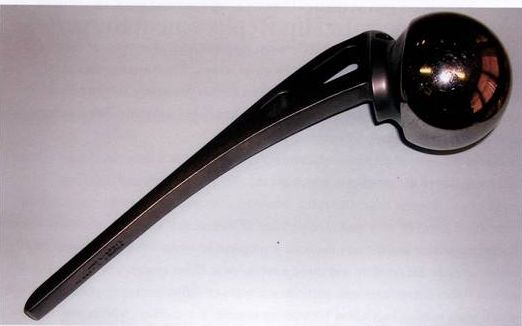
Austin Moore hemi-arthroplasty (for fracture of the femoral neck in
elderly low demand patients. Still in use.
Knowles Pins
These were used in the percutaneous fixation of undisplaced fractures of the femoral neck, and are still occasionally used.
Three Knowles pins as used in undisplaced femoral neck fracture
-o0o-
